ANAESTHESIA AND INTENSIVE CARE LECTURES,PROCEDURES CASE DISCUSSIONS AND OTHER TOPICS IN ANAESTHESIA AIMED AT PRACTISING ANAESTHETISTS AND RESIDENTS
DISCLAIMER
The contents of this blog are solely meant for information & education purpose only.These may be the basis of actual treatment, but not necessarily. Information from other websites and journals are also included. So the author is not responsible for any inaccuracy,loss, or damage that may arise due to the use of these informations published here. I do respect copyright & always give credits to the original author(s) and thankful to them. Inspite of my utmost effort and care there can be human error. If anyone finds any violation of copyright please inform me at anesthesiatoday@gmail.com and necessary action will be taken soon as possible. My blog is also non-commercial.
Back to the basics!!! Safe conduct of anaesthesia should be the priority when surgical cases are posted for procedures.The expertise and experience of the anaesthetist along with proper monitoring are essential in achieving this goal, but without considering the basics of anaesthesia practise even an experienced physician backed up by all essential monitors may turn to be a dangerous anaesthetist. Here are the ten golden rules of anaesthesia which stand immortal even in the midst of recent advances.
1.Assess and prepare the patient adequately:So that you will not anaesthetise anyone with multisystem disorders, heart disease,anemia or metabolic disorders.The physician should get sufficient information about the medications the patient is receiving as the drug interaction of these drugs with anaesthetic agents are complex and sometimes dangerous.Prepare the patient by correcting dehydration, severe anaemia,diabetes, heart failure,hyperthyroidism etc..Identifying pre existing diseases and correcting them help the anaesthetist for proper risk stratification of cases and a proper plan of anaesthesia technique can be made.The detailed explanation of the anaesthesia procedure must be offered to the patient and an informed consent must be obtained.
2.Starve the patient even for local anaesthesia: So that if the patient tries to vomit his stomach is less likely to be full. In case the local anaesthesia fails or a toxicity or CNS involvement by the local anaesthetics he may have to administer general anaesthesia or to resuscitate the patient.
3.Anaesthetise him on a tipping table: Because he may still vomit ,even if he is supposed to have been starved.So you must be able to tip him head down.If you do this, the chance of aspiration (even if he regurgitates)is very less.
4.Check your drugs and equipment: Before your start,especially if you are using less simple equipment. The equipment to preserve his airway must be ready beside you.All drugs including drugs for emergency use must be loaded and labelled.The anaesthesia machine and monitors should be checked as per routine checking protocols.
5.Keep a sucker instantly ready: Tested and working,so that if his pharynx fills with vomit,you can suck it out.You will also need suction catheters.A properly working suction catheter is mandatory for administering anaesthesia.
6.Keep airway clear: Because it can be easily obstructed.One way to do this is to use a Guedel's airway.You will need a range of different sizes. Alternatively you can use the triple manuevour too. Recently with the introduction of LMAs the airway management has become simpler and easier.
7.If the patient needs ventilation: Have a self inflating bag, non re breathing valve,and a face mask ready.You may need to intubate the patient.Have access to laryngoscope, tracheal tubes,an introducer and suction catheters.Intubation is the only way you can be sure to control his airway and prevent aspiration.
8.Have a vein open: Because if the patient has a drip,or an indwelling needle you can treat some of the complications ,that may arise during anaesthesia more easily, and give him both blood and fluids quickly.An open vein is an essential precaution in all major operations.
9.Monitor pulse and blood pressure: Continually during the operation and immediately after it,so that you are able to take the the necessary corrective action before it is too late.You must recognise cardiac arrest immediately.One of the most effective ways to do this is to strap a precordial stethescope to his chest and listen to the sounds.(we have advanced to the level of TEE now)
10.Always have someone in the room who can apply cricoid pressure: Some body who is experinced in giving cricoid pressure effectively must be available in the operating room.He should be either a second anaesthetist or a nurse anaesthetist.The practise is useful in emergency and to anaesthetise full stomach patients.Now the practise of cricoid pressure is a controversial issue as some physicians believe it will do more harm than good .They argue that the pharyngeal stimulation may result in regurgitation and it is difficult to estimate the required pressure.Also placement of LMA is difficult and chance of tracheal cartilage injury is high..
These Golden rules were published in the beginning of anaesthesia practise aiming to help the anaesthetist to deliver safe anaesthesia but many of the rules stated are applicable to modern days of practise as well..The anaesthesiologist should not forget the directive primum non nocere (“first of all do no harm”) and should always observe the basics, guidelines and protocols in spite of advanced monitoring.Let us remember the saying
‘Provide good care with very few monitors’
‘More monitoring, however does not necessarily lead to better care’
‘No monitor can ever replace a human being as he has the 6th sense.’
‘The focus of attention for greater part of the time should be on the patient and the operation, not on monitors.’
- Wendell C. Stevens
Ref: 1) Primary Anaesthesia Edited by Maurice King, Oxford University Press 1992
The American Society of Anaesthesiology classification of physical status(ASA) is still used widely as a scoring system to assess the fitness of patients subjected to anaesthesia and surgery. The scoring system was devised to assess the physical status of patients before anaesthesia is planned and was applied uniformly for all patients.The grading system was useful for record keeping and for statistical analysis of patients' health status who were scheduled for administration of anaesthesia.This grading system is not indicated for prediction of operative risk.
The evolution of ASA grading system[1]
In 1940-41, ASA asked a committee of three physicians (Meyer Saklad, M.D., Emery Rovenstine, M.D., and Ivan Taylor, M.D.) to study, examine, experiment and devise a system for the collection and tabulation of statistical data in anaesthesia which could be applicable under any circumstances.[1] They were given the task to devise a grading system to assess the operative risk , but after detailed studies research and discussion they stated that "In attempting to standardize and define what has heretofore been considered 'Operative Risk', it was found that the term ... could not be used. It was felt that for the purposes of the anesthesia record and for any future evaluation of anesthetic agents or surgical procedures, it would be best to classify and grade the patient in relation to his physical status only."They described a six-point scale, ranging from a healthy patient (class 1) to one with an extreme systemic disorder that is an imminent threat to life (class 4). The first four points of their scale roughly correspond to today's ASA classes 1-4, which were first published in 1963.[2] The original authors included two classes that encompassed emergencies which otherwise would have been coded in either the first two classes (class 5) or the second two (class 6).Two modifications were made in 1963 when the new classification is proposed ,the previous classes 5 and 6 were removed and a new class 5 was added for moribund patients not expected to survive 24 hours,with or without surgery.In addition emergency cases were designated by the letter 'E'.[3] The sixth class is a recent addition for declared brain dead organ donors. The six ASA classes for evaluation of physical status are
ASA I
An immediate green flag: Normal healthy patients are coming under this group.Ptients can walk one flight of stairs or two level city blocks without distress.No clinical co morbidity , no significant past or present medical or surgical history.
ASA II
Patients have mild to moderate systemic disease which is well controlled.Patients are able to walk up one flight of stairs or two level city blocks,but with moderate levels of exertional distress. History of well-controlled disease states including non-insulin dependent diabetes,Patients with anginal symptoms less than once a week,High blood pressure treated with a single type of medicine,[4],or asthma controlled by inhalers. ASA III
Patients with severe systemic disease that limits activity, but is not incapacitating.Angina symptoms more than once a week,Taking more than one blood pressure tablet Having complications of diabetes such as kidney failure or poor circulation,Asthma requiring frequent hospital admissions,Respiratory disease [COPD / COAD] causing breathlessness climbing a single flight of stairs,Someone with a raised creatinine of less than 200 micro mol/L,without dehydration, are all examples.[5]
ASA IV
A Patient with severe systemic disease that is a constant threat to life:Advanced liver disease, severe COPD, ARDS, History of unstable angina pectoris, myocardial infarction or cerebrovascular accident within the last six months, severe congestive heart failure, , and uncontrolled diabetes, hypertension, epilepsy,etc.
ASA V
A moribund patient not expected to survive 24 hours with or without surgery, eg;Severe gangrenous intestine in septic shock or terminally ill patients.
ASA VI A brain dead donor for organ harvestation.
The prefix 'E' is added to emergency operation of any class eg; ASA I E, for emergency caesarean section in an ASA I patient.
The inconsistency and inadequacy of ASA grading system has been questioned for many years. The major drawbacks of this grading system are
Inconsistency of grading between anesthetists.[6],Research by Haynes, S. R. and Lawler, P. G. P, showed that so much variation was observed between individual anaesthetist's assessments when describing common clinical problems and that the ASA grade alone cannot be considered to satisfactorily describe the physical status of a patient.
Age; is not considered as an influencing factor,extremes of age like elderly patients and neonates may have poor tolerance to surgery and anaesthesia in the absence of systemic illness and cannot be considered as ASA 1 patients.
The grading system is not well suited for assesing physical status of special clinical conditions like burns,trauma and metabolic disorders
No grade was available to describe moderate systemic illness.
The ASA Grading System shows poor interrater reliability in pediatric practice[7]
Here comes the importance of revising the ASA physical status system.An attempt was made by Tomoaki Higashizawa M.D., Ph.D. and Yoshihisa Koga M.D.,who revised the score and introduced a 7 graded scoring system.This was done by modification of the original ASA grading system as below.[8] The authors claim reevaluation of ASA physical status (7-grade) can provide a better grading outcome for predicting the incidence of intra- and postoperative complications in surgical patients compared with the conventional ASA's.
With 2 subclasses 1a 1b,2a,2b this classification seems to be appropriate to fill up the gap between the severity of systemic illness but difficult to apply for routine use because of its complex nature.We expect that a revision of ASA grading system will be implemented soon by ASA.
Many anaesthetists are concerned more with the morbidity and mortality of associated risk conditions, The physical status evaluation alone was not useful for risk stratification and many other grading systems were devised to evaluate the perioperative risk.eg; E-PASS and POSSUM score.
Reference:
1)Saklad M. Grading of patients for surgical procedures. Anesthesiology 1941; 2:281-4.(by courtesy of WIKIPEDIA) 2)Little JP (1995). "Consistency of ASA grading". Anaesthesia50 (7): 658–9. pubmed. 3)New classification of physical status. Anesthesiology 1963; 24:111 4)Margaret J. Fehrenbach, RDH, MS, from the American Society of Anesthesiologists, Medical Emergencies in the Dental Office (Malamed, Mosby, 2008), 5)http://www.nhfd.co.uk/003/hipfractureR.nsf/ (National hip fracture database) 6)Haynes, S. R. and Lawler, P. G. P. (1995), An assessment of the consistency of ASA physical status classification allocation. Anaesthesia, 50: 195–199. 7)Aplin S, Baines D,Lima, Use of the ASA physical status grading system in pediatric practice.,Pediatric Anaesthesia,2007 Mar;17(3):216-22. 8)T. Higashizawa & Y. Koga : Modified ASA Physical Status (7 grades) May Be More Practical In Recent Use For Preoperative Risk Assessment . The Internet Journal of Anesthesiology. 2007 Volume 15 Number 1.
A 30 year old ASA 1 patient weighing 70 kg is scheduled for open reduction and internal fixation of fracture both bones on right upper limb. The pre anaesthetic check up was unremarkable except for mild nasal allergy.The patient received 3 mg intravenous midazolam in operation theatre for sedation and an interscalene brachial plexus block was attempted by the anaesthetist using 20 ml 1% lignocaine along with 20 ml 0.25% bupivacaine.Analgesia was adequate and almost complete after 10 minutes of the block and the surgeon was about to operate. The patient complained of dizziness and vomited once.The blood pressure dropped below70 mm Hg systolic and the pulse was felt slow, feeble and thready. The chest on auscultation revealed equal and bilateral air entry. Later on he complained of numbness of the face and began to convulse. Immediate support of airway and ventilation provided by mask ventilation and intubation after intravenous thiopental. Intravenous fluids administered and intravenous ephedrine given at increments . Blood pressure dropped further down and patient had a cardiac arrest following asystole. CPR given as per ACLS protocols and a lipid emulsion was requested. The patient responded to resuscitative efforts and intralipid administration was not necessary. He was shifted to intensive care unit for close monitoring of vitals and has fully recovered without any neurologic sequelae.
Local anaesthetics are drugs used to prevent or relieve pain in specific regions of the body without producing unconsciousness. They block pain sensation by blocking conduction of pain impulses through nerves.Motor blockade and autonomic blockade are also observed as part of local anaesthetic action.Local anaesthetic drugs are widely used in dentistry and surgical specialities for providing surface anaesthesia, infiltrative anaesthesia or for nerve block. They are indispensable for the anaesthetist, in providing Regional Anaesthesia.The drug lignocaine find an unique place in crash cart for CPR and in emergency medicine trolley for treating arrhythmias.No pain management services can run without using local anaesthetics.However precaution must be taken while using them as chances of toxicity or side effects are high and may even be fatal. Manifestations of toxic reaction may range from minor urticaria or edema to very severe neurological toxcity or severe cardiovascular collapse.So basic resuscitation equipments and essential drugs should be kept ready before administering LAs to any patient. A brief review of local anaesthetic toxicity and its management, is given here. Pharmacology: Structurally, all local anaesthetics are similar and consist of three parts: a lipiophilic (aromatic) end, a hydrophilic (amine) end, and a link between the two ends.[1] This intermediate link can be either an aminoester or an aminoamide bond, which classifies the local anaesthetics into two different groups: amides and esters. Esters include Procaine, Cocaine, Chlorprocaine, Amethocaine, etc .Amides include Lignocaine, Bupivacaine, Levobupivacaine, Ropivacaine etc.
All local anaesthetic drugs are weak bases and exists in an equilibrium between ionised and non ionised forms in solution.The non-ionised form diffuses readily across the neuronal membranes into the axoplasm, where it ionises and blocks sodium channels within the cell.
Factors affecting the anaesthetic activity of local anaesthetics include the dissociation constant (pKa),[2]
protein binding, lipid solubility, pH, and vascularity at the injection site.The pH at which the amount of ionised and nonionised drug is equal is known as the pka or diffusion constant , (the pKa of lignocaine is 7.8 but at a pH of 7.4, more than half of the drug exist as charged cation) The onset of action of the drug is determined by the dissociation constant and pH of the medium. Anaesthetic with a pKa value near the physiological pH has a greater proportion of drug in the non-ionised form. The non ionised form diffuses more readily across the nerve sheaths and membrane to its site of action. Therefore, local anaesthetics with pKa values close to physiological pH tend to have a more rapid onset of action as the non ionised content of the drug is more. Factors that promote local extracellular acidosis (eg: infection) increase drug ionisation and therefore reduce local anaesthetic diffusion and penetration of the nerve membrane. Addition of sodium bicarbonate (1 ml 8.4% sodium bicarbonate per 19 ml 1 % lignocaine)to local anaesthetics increases the pH of the solution, which increases the ratio of non-ionised to ionised form,resulting in a more rapid onset of action. The potency of local anaesthetics is affected by its lipid solubility A highly lipid-soluble drug readily penetrates cell membranes and thus have higher potency compared to drugs having lower lipid solubility
The degree of protein binding( alpha 1 acid glyco protein) and vascularity also affects the local anaesthetic’s
duration of action. Those with high plasma protein binding have longer durations of action. Addition
of a vasoconstrictor like epinephrine to lipid soluble local anaesthetics decreases vascularity at the injection site, which prolongs the duration of action (via reduced absorption of the drug into the systemic circulation).
Mechanism of action:
LAs are membrane-stabilising drugs that reversibly decrease the rate of depolarisation and repolarisation of excitable membranes.Local anaesthetics block sensory and motor function by impeding the permeability of
neuronal cell membranes to sodium. This action prevents the rapid influx of sodium during the depolarisation phase of the action potential and its onward transmission.LAs selectively bind to inactivated closed sodium channels and stabilise them in order to prevent channel opening due to nerve stimulation and subsequent propagation of action potential.The primary electrophysiological effect of these compounds is to cause a local decrease in the rate and degree of depolarisation of the nerve membrane such that the threshold potential for transmission is not reached and the electrical impulse is not propagated down the nerve.[2]
Metabolism: The ester type local anaesthetics are hydrolysed by esterases in tissues and blood, while the amide types are metabolised primarily in the liver by cytochrome P450 enzymes and then excreted through kidney. Dosage adjustments may be made in hepatic and renal failure.[2]
Calculation of percentage and dosage:
Concentration. Drug concentration is expressed as a percentage, i.e. grams per 100ml (e.g. 1%=1 g/100 ml (1 000 mg/100 ml) or 10 mg/ml). (Bupivacaine 0.25%=2.5 mg/
ml; lignocaine 1%=10 mg/ml.)
Dilution. When adrenaline is combined in an anaesthetic solution the result is expressed as a dilution (e.g. 1:100 000):
• 1:1 000 means 1 mg/1 ml (0.1%)
• 1:10 000 means 1 mg/10 ml (0.01%)
• 1:2 000 means 1 mg/2 ml (0.05%)
• 1:20 000 means 1 mg/20 ml (0.005%)
• 0.1 ml of 1:1 000 adrenaline added to 10ml of anaesthetic solution = 1:100 000 dilution or 0.01 mg/ml
• 50 ml of lignocaine 1% with adrenaline 1:100 000 contains lignocaine 500 mg and adrenaline 0.5 mg.
Adrenaline is the most commonly used vasoconstrictor, it is added to local anaesthetic solutions in concentrations ranging from 1 in 80,000 to 1 in 300,000, although most are usually prepared to contain a 1 in 200,000 (5 microgram /ml) concentration of adrenaline.[3]
Practical Point
Adrenaline 1:1000 contains 1 gram of adrenaline per 1000mls solution i.e. 1mg/ml. To prepare a 1 in 200,000 solution the 1:1000 must be diluted 200 times. This is achieved by taking 0.1ml (= 0.1mg) and adding 19.9 mls of local anaesthetic solution.
Etiology of toxic reactions to Local Anaesthetics:[1]
Systemic: CNS and CVS toxicity, termed as local anaesthetic systemic toxicity or LAST
Local toxicity: Neuronal damage or skeletal muscle damage
Others: Methemoglobinemia (prilocaine) Hydrolysis of prilocaine initially leads to the formation of o-toluidine products that bind to haemoglobin and oxidises Hb to ferric form and cause methaemoglobinaemia.
Allergy: Allergic reactions are rare even though IgE mediated reactions can occur and may be seen with ester linked LAs.
Addiction: Cocaine may lead to drug dependance.
Reaction to vasoconstrictors: Tachycardia, hypertension, headache,apprehension, which usually need no treatment.
Vasovagal reaction: Rapid onset of bradycardia, hypotension, pallor,faintness.Usually seen when patient assumes sitting position.
Anaphylaxis: Hypotension, bronchospasm, urticaria, oedema, needs treatment as per anaphylaxis algorithm
Transient nerve damage like persisting paraesthesia, prolonged anaesthesia etc will resolve spontaneously and permanent nerve damage is rare.
Local anaesthetic systemic toxicity (LAST)
Toxicity may occur due to[2]
Accidental intravascular or intrathecal injection
Relative overdosage of drug used
Rapid systemic absorption from the injected site
CNS Toxicity:Symptoms and signs of CNS toxicity are manifested as initial excitation followed by depression. The pre excitation phase is characterised by tinnitus, light headedness ,confusion and circum oral numbness and paraesthesia. This progresses on to the excitation phase where the signs are shivering, tremor muscular twitchings and convulsions .The final stage of depression is fatal as patients may loose consciousness and may go in for respiratory arrest. Blockade of inhibitory pathways and inhibition of release of glutamate in cerebral cortex produce initial excitation.Blockade of inhibitory pathways allows facilitatory neurons to function in an unopposed fashion, which results in an increase in excitatory activity leading to convulsions. A further increase in the dose of local anesthetic leads to inhibition of activity of both the inhibitory and facilitatory circuits, which results in a generalized state of CNS depression.Respiratory or metabolic acidosis increases CNS toxicity by increased cerebral blood flow and resulting in rapid delivery of anaesthetic agents to brain.Acidosis also decreases intracellular pH resulting in iron trapping, decreases the plasma protein binding making available more free form of the base. Seizures produce hypoventilation and a combined respiratory and metabolic acidosis, which further exacerbates the CNS toxicity. Hence immediate support of airway with proper ventilation and meticulous control of seizures advised,in LA toxicity
CVS Toxicity: Direct cardiovascular effects and direct peripheral vascular effects are observed .The direct CVS effects include bradycardia due to action on sodium channels which reduces action potential duration and effective refractory period.They increase PR interval and QRS complex duration resulting in prolongation of conduction time.They also exert dose-dependant negative inotropic action on cardiac muscle.Local anesthetics may depress myocardial contractility by affecting calcium influx and triggered release from the sarcoplasmic reticulum,[2] The direct peripheral vascular effects include a biphasic response on vascular smooth muscles characterised by initial vasoconstriction followed by vasodilatation.Thus there will be a reduction in blood pressure. The toxic effects are more pronounced with bupivacaine and remain sustained.Ventricular arrhythmias including fibrllation are more common with bupivacaine and cardiac resuscitation is more difficult after bupivacaine-induced cardiovascular collapse, and acidosis and hypoxia markedly potentiate the cardiotoxicity of bupivacaine.(4)
Treatment of LAST:
In 2007, the Association of Anaesthetists of Great Britain and Ireland published guidelines for the
management of severe local anaesthetic toxicity.[5] In 2008, the American Society of Critical Care Anesthesiologists and the American Society of Anesthesiologists Committee on Critical CareMedicine,[6] as well as the Resuscitation Council of the United Kingdom[7] also published protocols for the treatment of LAST. In 2010, the American Society of Regional Anesthesia and Pain Medicine published its practice advisory on LAST.[8] These guidelines emphasise the importance of airway management and early cardiopulmonary resuscitation, They also strongly advise use of lipid emulsions along with resuscitative measures and have incorporated the use of lipid emulsion therapy in their guidelines, in the management of LAST. The AAGBI algorithm is shown below.
What is intra lipid? How it helps?
Intralipid is a brand name for the first safe fat emulsion for human use, approved in 1962 in Europe and invented by Professor Arvid Wretlind, Sweden. It is used as a component of parenteral nutrition for patients who are unable to get nutrition via an oral diet. It is an emulsion of soy bean oil, egg phospholipids and glycerin. It is available in a 10%, 20% and 30% concentration. The 30% concentration is not approved for direct intravenous infusion, but should be mixed with amino acids and dextrose as part of a total nutrient admixture.Intralipid provides essential fatty acids, Linolenic acid (LA), an omega-6 fatty acid,alpha-linolenic acid(ALA), an omega-3 fatty acid. Some preparations of the anaesthetic drugs propofol and etomidate (the vehicle for etomidate is propylene glycol) are supplied using Intralipid as a vehicle.[9] Intralipid is widely and freely available in all hospital intensive care units as this is one of the major constituent of parenteral nutrition
In 1998 Weinberg et al[10] first reported that lipid emulsion infused during resuscitation increased the
median lethal dose (LD50) of bupivacaine in rats by 50%. Followed by in 2006 Rosenblatt et al[11] and
Litz et al[12] reported successful clinical use of lipid emulsion to reverse local anaesthetic induced cardiac
arrest.Many clinical reports released after this supported the use of lipid emulsion in the management of LAST[13,14,15] caused due to bupivacaine, levobupivacaine, and ropivacaine.
The exact mechanism of action of lipid emulsion therapy is not known. It may serve as a“lipid sink”, providing a large lipid phase in the plasma, enabling capture of the local anaesthetic molecules and making them unavailable to tissues.Alternatively they prevent impaired fatty acid delivery caused by local anaesthetics in the mitochrondria, and enhance energy production. The commonly used lipid emulsion preparation is Intralipid 20%, and the efficacy of other preparations is not studied in detail . Propofol is not asuitable substitute for Intralipid. It is formulated in a 10% lipid emulsion as the amount of lipid emulsion is less compared to the concentration of propofol and higher doses of propofol have direct cardiovascular depressant effects. The recommended Intralipid regimen as given by AAGBI, entails an initial intravenous bolus injection of a 20% emulsion at 1.5 mL/kg over 1 minute, followed by an infusion of 15mL/kg/h. Cardiopulmonary resuscitation should be continued. If cardiovascular stability is not restored after 5minutes or if haemodynamics deteriorate, a maximum of two repeated boluses (1.5 mL/kg) may be given at 5-minute intervals. The intravenous infusion rate should also be doubled to 30 mL/kg/h. A maximum of three boluses can be given, and a cumulative dose of 12 mL/kg should not be exceeded.
It is seen that increasing the dose beyond 8 mL/kg is unlikely to be useful and in practice, resuscitation of an adult weighing 70 kg is as follows:
Use a 500-mL bag of fat emulsion (Intralipid 20%) and a 50-mL syringe.
Draw up 50 mL and give it stat intravenously, and then draw up and give another 20 mL.
Do exactly the same thing up to twice more as the epinephrine is given—if necessary or appropriate.
Then, attach the fat emulsion bag to a giving set and administer it intravenously over the next 15 minutes.
Contra-indications to lipid emulsion therapy include lipid metabolism disorders and egg allergy, and caution is required for patients with anaemia, severe liver disease, coagulopathy, and pulmonary disease. Potential complications include allergic reaction, fluid overload, impaired liver function, hypercoagulability and pancreatitis.
Here is the great and eminent personality whom i admire and salute, Dr. Weinberg,a pioneer behind this experimentation and who first postulated that lipid emulsion has a role in the treatment of LA toxicity. Following his second report in 2003 stating that "Lipid emulsion infusion rescues dogs from bupivacaine-induced cardiac toxicity"., published in Regional Anesthesia and Pain Medicine 2003; 28: 198-202, many case reports have been published in support of the efficacy of lipid emulsions for reversing local anaesthetic toxicity.[13,14,15] He himself has designed a web site and shared his experience knowledge and invited people from all over the world for contributions in this regard .The site deals with local anaesthetic toxicity, literature, case reports,experiments, and treatment regimen.He has designed the lipid rescue kits and is running a laboratory for further research on this issue watch this site: www.lipidrescue.org This figure shows a Home made lipid rescue kit .This kit designed by Mike Alway, RPh, from BonSecours Hospital. "The container for the kit is a blue storage bin that has a clear hinged lid. It contains the 20% Lipid bag (500 ml), IV tubing, 60cc Syringes (2), and needles. The protocol is attached to the Lipid bag inside the kit and also pasted it on the outside.
So make your own rescue kits today and keep them in OR within your reach.
Reference:
1.KC Lui;YF Chow, Safe use of local anaesthetics: prevention and management of systemic toxicity; Hong Kong Med J 2010;16:470-5
2. Miller's Anaesthesia,7th edition, R D Miller et al , Churchil Livingston
3.René du Plessis, MB ChB,Specialist Anaesthetist,Bloemfonte, Local anaesthetics: Characteris tics, uses
and toxicities;CME September 2009 Vol.27 No.9
4.Englesson S: The influence of acid-base changes on central nervous system toxicity of local anaesthetic agents. An experimental study in cats. Acta Anaesthesiol Scand 1974; 18:79-87.
5.Guidelines for the management of severe local anaesthetic toxicity. The Association of Anaesthetists of Great Britain &Ireland; 2007.
6.Gabrielli A, O’Connor MF, Maccioli GA. Anesthesia Advanced Circulatory Life Support. The American Societyof Critical Care Anesthesiologists & The American Society of Anesthesiologists, Committee on Critical care Medicine;2008.
7.Cardiac arrest or cardiovascular collapse caused by local anesthetic. Resuscitation Council (UK); 2008.
8.Neal JM, Bernards CM, Butterworth JF 4th, et al. ASRA practice advisory on local anesthetic systemic toxicity. RegAnesth Pain Med 2010;35:152-61.
9.Wikipedia, en.wikipedia.org/wiki/Intralipid. 10.Weinberg GL, VadeBoncouer T, Ramaraju GA, Garcia-Amaro MF, Cwik MJ. Pretreatment or resuscitation with a lipid infusion shifts the dose-response to bupivacaineinduced
asystole in rats. Anesthesiology 1998;88:1071-5.
11. Rosenblatt MA, Abel M, Fischer GW, Itzkovich CJ, EisenkraftRosenblatt MA, Abel M, Fischer GW, Itzkovich CJ, Eisenkraft JB. Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest.Anesthesiology 2006;105:217-8.
12.Litz RJ, Popp M, Stehr SN, Koch T. Successful resuscitation of a patient with ropivacaine-induced asystole after axillary plexus block using lipid infusion. Anaesthesia 2006;61:800-1.
13.Julio A. Warren, MD,R. Brian Thoma, MD, Alexandru Georgescu, MD,Saurin J. Shah, MD
Intravenous Lipid Infusion in the Successful Resuscitation of Local Anesthetic-Induced Cardiovascular
Collapse After Supraclavicular Brachial Plexus Block (Anesth Analg 2008;106:1578 –80)
14.Meg A. Rosenblatt, M.D., Mark Abel, M.D., Gregory W. Fischer, M.D.,Chad J. Itzkovich, M.D.,James B. Eisenkraft, M.D; Successful Use of a 20% Lipid Emulsion to Resuscitate a Patient after a Presumed Bupivacaine-related Cardiac Arrest
15. R. J. Litz,M. Popp,S. N. Stehr, Anaesthesia, Volume 61, Issue 8, pages 800–801, August2006, Successful resuscitation of a patient with ropivacaine-induced asystole after axillary plexus block using lipid infusion.
CEB is a commonly performed anaesthetic procedure to provide intra operative and postoperative analgesia in children undergoing lower limb and abdominal surgeries. It is a simple and highly effective technique useful for most of the surgical procedures of the lower half of the body, like urinary tract surgeries,circumcision, herniorrhaphies, orthopedic surgeries on the lower limb and pelvis, or operations of the anus or rectum.Excellent surgical conditions are obtained in congenital talipus equino varus(CTEV) surgery when combined with light general anaesthesia.The technique can be successfully used in children, as the fluidity of the epidural fat is more compared to adults, allowing easy spread of the deposited solution. Moreover if lumbar or thoracic anaesthesia is required, an epidural catheter can be threaded and advanced easily to achieve analgesia at the desired dermatomal level.
Anatomical Landmarks:
The sacrum is a large triangular piece of bone formed by fusion of the 5 sacral vertebrae. The lamina of the fifth and mostly of the 4th vertebra fails to fuse in the midline creating a deficiency known as sacral hiatus, which can be palpated by running your finger upwards tracing the segments of the coccyx from below. The hiatus can be easily palpated in children as the land marks are more clear. The contents of the sacral canal include[1]
The sacral and coccygeal nerves with their dorsal root ganglia
The terminal part of the dural sac which ends between S1 and S3 and from where the pia mater extends downwards as filum terminale.
A venous plexus formed by the extension of internal vertebral plexus.
loose areolar and fatty tissue.
The filum terminale - the terminal fibres of the spinal cord which does not contain nerves. This exits through the sacral hiatus and is attached posterior to coccyx.
Pediatric considerations: In infants or small children sacrum is cartilaginous which can allow for inadvertent intra-osseous injection.Also the spinal cord reaches L3-4 in the neonate and the dural sac can be found at S3-4. This increases the risk of inadvertent dural puncture or spinal cord injury. Adult levels of L1 and S1 are usually reached by 1 year of age. Up to 6-7 years of age good results are observed.As the age advances the axis of the sacrum in relation to the lumbosacral spines changes and the hiatus is difficult to access or even fuse. The sacrococcygeal ligaments are tough or calcified.Hence the procedure may be difficult in adulthood.
The volume of the sacral canal averages 14.4 mL, but varies from 9.5 to 26.6 mL.
Drugs and dosages: Most commonly used drugs are lignocaine and bupivacaine Additives may be used to enhance analgesia, relaxation or prolongation of effect.For practical purposes the dosage suggested by Armitage may be used which is simple and easy to remember.
Armitage Formula:
Bupivacaine, max dose 2.5 mg/kg without adrenaline and 3mg/kg with adrenaline(1:200000)
0.5 ml/kg for a lumbosacral block
1 ml/kg for a thoraco-lumbar block
1.25 ml/kg for a midthoracic block
(0.25% Bupivacaine up to a maximum of 20ml, for analgesia and 0.5% if motor block is desired.)
Lignocaine max dose 7mg/kg without adrenaline and 10 mg/kg with adrenaline
0.5 ml/kg for lumbosacral block
1ml/kg for thoracolumbar block
1.5 ml/kg for mid thoracic block
(Maximum of 20ml, 1% for analgesia and 2 % for motor block)
If more than 1ml/kg (to a maximum of 20 ml) needs to be given it is preferable to avoid caudal route and go for a higher epidural route(for lesser volume of drug) as it is observed that large volumes of caudal drug spread rostrally above T4. According to bromage;[2] anesthetic dose requirements are about 0.1 mL/ segment/year of age for 1% lidocaine or 0.25% bupivacaine.
Scott’s Calculation:
Calculates the dose based on the child’s age and/or weight table.If the child is of average weight for his or her height, both figures will be the same.Avoid this formula in obese children to prevent overdosage.
In premature infants successful caudal anaesthesia can be performed with 1 mL/kg of 0.375% bupivacaine, for surgeries like inguinal herniorrhaphy, orchiopexy, and circumcision.
Identification of the sacral hiatus and the procedure of the block:
The procedure must be carried out under strict aseptic precautions,
Patient position:
Lateral position in children or prone position (desirable) for adults.The pelvis is elevated with the help of a pillow and the thighs are little extended The legs turned in wards,(internally rotated ). This makes the identification of the hiatus more easy by relaxing gluteal muscles. Look at figure 2B.
The standard technique as described by Miller is shown below:[3]
Caudal anesthesia requires identification of the sacral hiatus. The sacrococcygeal ligament (i.e.,extension of ligamentum flavum) overlying the sacral hiatus lies between the sacral cornua. To facilitate locating the cornua, the posterior superior iliac spines should be located and, by using the line between them as one side of an equilateral triangle, the location of the sacral hiatus should be approximated After the sacral hiatus is identified, the index and middle fingers of the palpating hand are placed on the sacral cornua,
and the caudal needle is inserted at an angle of approximately 45 degrees to the sacrum.
While advancing the needle, a decrease in resistance to needle insertion should be appreciated as the needle enters the caudal canal. The needle is advanced until bone (i.e., dorsal aspect of the ventral plate of the sacrum) is contacted and then slightly withdrawn, and the needle is redirected so that the angle of insertion relative to the skin surface is decreased. In male patients, this angle is almost parallel to the coronal plane; in female patients, a slightly steeper angle (15 degrees) is necessary. During redirection of the needle and after loss of resistance is again encountered, the needle is advanced approximately 1 to 2 cm into the caudal canal.
Performance of caudal block.[6] SC, sacral cornua; PSIS, posterior superior iliac spine; SH, sacral hiatus; TC, tip of coccyx. Note that an equilateral triangle is formed with the fingertips from PSIS to PSIS to needle insertion at SH.(By courtesy of Cristian TANASE,Clinical Emergency Hospital for Children “GrigoreAlexandrescu” Bucharest.)
Further advance is not attempted because dural puncture and unintentional intravascular cannulation become more likely. One method of increasing the likelihood of correct caudal needle placement is to inject 5 mL of saline rapidly through the caudal needle while palpating the skin overlying the sacrum. If no midline bulge is detected, the needle is probably positioned correctly. In contrast, if a midline bulge is detected during saline injection, the needle is positioned incorrectly.
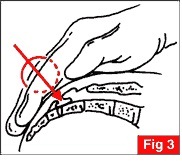
Simple teaching: [2] The sacral hiatus can be located by first palpating the coccyx, and then sliding the palpating finger in a cephalad direction until a depression in the skin is felt. Once the sacral hiatus is identified the area above is carefully cleaned with antiseptic solution, and a 22 gauge short bevelled cannula or needle is directed at about 45° to skin and inserted till a "click" is felt as the sacro-coccygeal ligament is pierced. The needle is then carefully directed in a cephalad direction at an angle approaching the long axis of the spinal canal.
1).Palpate the coccyx with the index finger of the left hand
2).Slide the palpating finger cephalad
3).Feel the depression.
4).Keep the finger at the hiatus and turn the hand at 80 degrees anchoring the index finger at the hitus
5).Hold the syringe filled with the drug in right hand.
1)Pierce the SC ligament by entering into it at 45 degree angle
2)Carefully advance and feel for the "click"
3)Once the click is felt lower the needle almost parallel to the coronal plane (along the long axis of the spinal canal)
4)Advance the needle further 1-2 cm into the caudal canal.
Instead of using the needle alone , a syringe filled with 1-2 ml saline may be attached to it.Once the caudal canal is entered, the saline can be injected freely without any resistance. Air should not be used for this loss of resistance technique as the incidence of air embolism is high in children.Once the canal is identified local anaesthetic test dose may be given to rule out accidental intravascular or dural puncture.
Continuous caudal anaesthesia may be given by inserting an epidural catheter through an indwelling cannula or a 20 gauge touhy needle used to puncture.Remember that the catheter can be threaded easily because of the fluidity of loose areolar tissues in children and catheter tip in mid thoracic or higher level may lead on to a higher level of block.Measuring the catheter with the length of spine may be used as a rough guide to decide on how far the catheter to be inserted.Tunnelling the catheter on the back using a touhy needle helps to secure the catheter and prevent fecal contamination of the entry site as well.
How to identify the caudal space and to ensure the correct placement of catheter.
Ease of injection by loss of resistance technique
Absence of a cutaneous bulging over the injection site
Test dose, A small amount of local anaesthetic should be injected as a test dose (2-4mls).Look for peri oral tingling or numbness,or hypotension Also look for lower lumbar segment motor block. If the test is negative proceed with injection.
Aspiration test for either CSF or blood.[2] A negative aspiration test does not exclude intravascular or intrathecal placement. The injection rate should not exceed 10 ml/30 seconds.[3] During injection also watch for acute toxicity
The whoosh test and modified swoosh test(see below)
Flouroscopy(see below)
Nerve stimulation test,the presence or absence of anal sphincter contraction to electrical stimulation is used as a guide for correct needle placement (using epidural nerve stimulators)
Ultrasound.(see below)
The whoosh test and modified swoosh test:[4]
The whoosh test is done by injection of air into the caudal epidural space with simultaneous auscultation over the thoracolumbar spine for an audible "whoosh" sound.Injection of air is associated with side effects like neurological complicaions and air embolism. So is being replaced by swoosh test where saline or the LA solution is used instead of air.1-1.5 ml of air or saline is used.
Fluoroscopy: is most commonly used in interventional spine procedures and is frequently used in confirming the location of caudal epidural needle[6]. It is necessary that caudal epidural needle placement should be confirmed by fluoroscopy alone or by epidurography when the procedure is used for caudal epidural injection of steroids for treating chronic pain syndromes.
Exposure to radiation is one hazard of flouroscopic confrmation and proper precautions to be taken.This include proper schielding, reducing exposure time and using pulsed imaging.
Ultrasound:Combined with fluoroscopy ultrasound gives almost 100% accuracy in placement of the needle.As an adjuvant tool ultrasound is useful along with other methods in difficult cases and when successful placement is mandatory.Ultrasound is radiation free, is easy to use, and can provide real-time images in guiding the caudal epidural needle into the caudal epidural space.[6]Sterile precautions are taken before probe placement and a transverse view of the sacral hiatus is made first by placing the transducer transversely at the midline over hiatus.The hiatus is seen as a hypoechoic region between two hyper echoic shadows, the SC ligament and the dorsal bony surface. Then a longitudinal view is made by keeping the transducer between the sacral cornua,and a needle is inserted and advanced under sonographic guidance in real time.The portion of the needle which entered into the canal may not be seen clearly.Again the transducer is rotated to view the transverse axis where the needle tip may be visualised as a small round hyper echoic structure between the two hyperechoic cornua and within the two hyper echoic bands formed by the SC ligament and the dorsal bony wall of sacrum. Images below are reproduced from Chen, Carl P. C. M.D.; Tang, Simon F. T. M.D,Anesthesiology:July 2004 - Volume 101 - Issue 1 - pp 181-184[7] where a detailed description of the procedure is available
Adjuvants used along with Local Anaesthetics: Adjuvants are used to intensify the block ,to reduce systemic absorption or to prolong the action.The commonly used adjuvants are,
Opioids :Prolong analgesia in infants and children but with attendant risks of respiratory depression and side effects like nausea vomiting and itching. It can produce urinary retention also. Hence morphine administration should be done under monitoring of vitals. Catheterization may sometimes be required. A dose of 50mcg/kg of preservative free morphine or diamorphine 30mcg/kg can be added to the local anesthetic solution[8].The optimal dose is between 33-50 μg/kg.[9] This will provide 12 to 24 hours of analgesia.Fentanyl 1-2 ug/kg may be also used but with unpredictable duration of action. Clonidine: An α2-adrenergic agonist,. A dose of 0.5-1.0 microgram/kg improves the quality and duration of analgesia without significant side effects[8]The analgesia may last upto 12 hours.Sedation and bradycardia are noted at doses above 5mic/kg. Ketamine: An NMDA antagonist. In doses of 0.25 - 1.0 mg/kg, causes significant prolongation of post operative analgesia, without significant side effects. May be combined with 0.25%bupivacaine.Preservative free ketamine is preferred. Higher doses (>0.5mg/kg) may produce neuroleptic side effects
Epinephrine: 5 mic/ml of epinephrine is used to detect intravascular placement of catheter or needle.It also prolongs the duration of action of LA by local vasoconstriction and thereby delaying uptake and metabolism. Continuous epidural anaesthesia: is possible by inserting a catheter into the caudal space, through an indwelling cannula or a touhy needle.The initial dose may be 0.05ml/seg/kg[10]
Less than 1 year of age 0.1-0.2ml/kg/hr of 0.1% bupivacaine
more than 1 year 0.1% bupivacaine with 3 microgram/ml of fentanyl at the rate of 0.1-0.4ml/kg/hr, (less than 0.5microgram/kg/hr of fentanyl to start with.)[11]Ropivacaine is used at the dose of 0.4mg/kg/hr
Pharmacological Considerations:
Local anaesthetics are classified into two groups, amides and esters. the amides are metabolised in liver while the esters are hydrolysed by esterases in the plasma.Since newborn and pediatric liver functions are immature and not fully functional the metabolism of amides is not complete and the un metabolised fraction can produce toxic reactions. Another factor which contributes to toxicity is the reduction in plasma proteins like albumin and alpha 1 acid glycoprotein resulting in excess free fraction of the drugs in plasma. On the contrary the volume of distribution of local anaesthetics is more in children compared to adults causing a reduction plasma concentrarion of these drugs and which may nullify the effect of reduced elimination allowing higher doses.For eg:The maximum safe dose of bupivacaine in neonates is 1.5mg/kg.Other Local anaesthetic drugs which may be used for caudal include Ropivacaine 0.2- 2 mg/kg and Levobupivacaine 0.25- 1 mg/kg with slight increase in duration of action.Pregnant patients need 25-35% reduction in dose requirements for labour analgesia due to engorged epidural veins reducing space.Caudal blockade in pediatrics is used primarily for perioperative pain control, whereas in adults it is primarily for chronic pain management. [12]
Combination with GA: For intra and post operative pain relief and to reduce the requirement of depressant general anaesthetic agents for rapid and smooth recovery, caudal is combined with GA, The procedure is ideal for children as positioning after induction is easy and the success rate is high. Inhalational or iv induction then securing airway with LMA or ETT, is followed by caudal injection.The disadvantage being, failure of detection of LA toxicity or high block in an anaesthetised child.Careful monitoring of vitals mandatory.The effectiveness of the block is determined by "loss of anal sphincter tone".[13]
Indications(Uses) :
Apart from the usual indications mentioned above the caudal block is highly useful for emergency surgical procedures like,testicular torsion, omphalocele correction,strangulated hernias,high risk neonates for anorectal and abdominal surgeries,biliary tract surgeries and operative procedures on stomach (especially when a catheter is threaded to deposit the drug at higher dermatomes)
Ambulatory and day care minor surgeries where fast-traching is desired.
For combining with General anaesthesia to provide stable hemodynamics, adequate analgesia and to reduce the requirement of general anaesthetic agents, in surgeries of abdomen, lower thorax or even open heart procedures.
Continuous epidural analgesia can be provided with a catheter in caudal space for long surgical procedures like orthopedic corrective surgeries or plastic surgery procedures of the lower limb.
Percutaneous epidural neuroplasty is a technique of administering local anesthetics, corticosteroids, hyaluronidase, and hypertonic saline through a caudal catheter for the purpose of lysing epidural adhesions. [13]
Advantages over conventional epidural anaesthesia:
Easy location because of the prominent anatomical landmarks, helps to establish the block faster
Reduced incidence of failed or patchy blocks
Predictable distribution of LA solution
Easy to place a catheter
Side effects:
Failed block , the incidence is as high as 5-20%.Ultrasound guidance helps to increase the success rate
Predominant unilateral block or patchy block. Lateralisation is due to rapid injection.
Dural puncture: due to anatomic variation and low lying dura in infants. Sequale is, a total spinal block with dilated pupils, apnea, and unconsciousness.
Local anaesthetic toxicity can be either due to intravascular injection or due to overdose resulting in excess plasma concentrations.Since the extradural veins have no valves, retrograde flow is fast once the drug is injected intravascularly.
Intra osseous injection
Bleeding
Introduction of infection.
Contraindications:
Patient refusal
local infections,eg: dermattis, pilonidal sinus
Coagulation disorders
Neurologic diseases,Poliomyelitis
Sensitivity to local anaesthetics
Increased intra cranial tension like meningitis, hydrocephalus etc.
Congenital malformations of lower meninges or spine eg: spina bifida, meningo myelocele
Management of Local Anaesthetic toxicity( in general:)[4]
Oxygenation, intubation, cardiac massage
Sodium bicarbonate hypertonic 4.2%(through central vein preferably) 2ml/kg/10 mts.(1mmol/kg/10mt) or isotonic 1.4% through peripheral vein 6ml/kg/10 mts(1mmol/kg/10mts)
IV midazolam or diazepam for seizures
IV atropine 0.02mg/kg
IV vasoactive agents, epinephrine 0.1ml/kg1/10000 solution (10 microgram/kg) or isoprenaline 0.1 mic/kg
Dopamine or dobutamine infusion 2-10 mic/kg/mt,
Calcium chloride 10-30 mg/kg
Treatment of VF/VT as per ACLS guidelines
Lipid emulsions IV.
Role of caudal block in pain management:
In radiculopathies refractory to routine management this route is adopted for pain relief. Percutaneous epidural neuroplasty uses a caudal catheter left in place for up to 3 days to inject hypertonic solutions into the epidural space to treat radiculopathy with low back pain and epidural scarring, typically from previous lumbar spinal surgery.[12]After confirmation of epidural space by fluoroscopy a mixture of drugs consisting of Local anaesthetics, steroids, hyaluronidase, and saline is injected.Initially1500 units ofhyaluronidase in 10mLof preservative-free saline is injected rapidly. This is followed by an injection of 10 mL of 0.2% ropivacaine and 40 mg of triamcinolone, An additional injection of 9 mL of 10% hypertonic saline is infused over 20 to 30 min. On the second and third days, the local anesthetic (ropivacaine) injection is followed up by the hypertonic saline solution. Antibiotic coverage is provided to reduce the possibility of epidural abscess formation.[12]. The video below illustrates how to conduct an ultrasound guided epidural instillation of steroids to treat chronic pain syndromes.
Cardiopulmonary Resuscitation is an emergency life saving procedure consisting of delivering effective chest compressions and effective ventilations to a victim of cardiac arrest. The American Society of Anesthesiology and European Resuscitation Council have made evidence based guidelines for the efficient and proper conduct of high quality CPR.These guidelines, being revised from time to time according to newer evidences, research and outcome help the primary care provider to offer the best care for the victims of cardiac arrest.The 2010 AHA Guidelines for CPR and ECC are based on an international evidence evaluation process that involved hundreds of international resuscitation scientists and experts who evaluated, discussed, and debated thousands of peer reviewed publications. Here is the new" guidelines(2010) in nutshell' for CPR from AHA .The major changes have been highlighted.A detailed information of both ERC and AHA Guidelines, is available from the resuscitation council links given below.
BASIC LIFE SUPPORT 1.Continued Emphasis on High-Quality CPR:
The 2010 AHA Guidelines for CPR and ECC once again emphasize the need for high-quality CPR, including
A compression rate of at least 100/min (a change from“approximately” 100/min)
A compression depth of at least 2 inches (5 cm) in adults and a compression depth of at least one third of the anteroposterior diameter of the chest in infants and children(approximately 1.5 inches [4 cm] in infants and 2 inches[5 cm] in children). Note that the range of 1½ to 2 inches is no longer used for adults, and the absolute depth specified for children and infants is deeper than in previous versions the AHA Guidelines for CPR and ECC
Allowing for complete chest recoil after each compression
Minimizing interruptions in chest compressions
Avoiding excessive(hyper) ventilation
There has been no change in the recommendation for a compression-to-ventilation ratio of 30:2 for single rescuers of adults, children, and infants (excluding newly born infants). The 2010 AHA Guidelines for CPR and ECC continue to recommend that rescue breaths be given in approximately 1 second. Once
an advanced airway is in place,rescue breaths can be provided at about 1 breath every 6 to 8 seconds (about 8 to 10 breaths/minute) and need not be synchronised with chest compressions which can be
continuous (at a rate of at least 100/min) 2.A Change From A-B-C to C-A-B
The major change made in BLS, from airway, breathing,and circulation the sequence has been changed to compression,airway and breathing .This is to aviod delay in delivering fast and effective chest compressions. Securing airway as the initial priority is time consuming and may not be 100% successful, especially by lone rescuers or paramedics.The vast majority of cardiac arrests occur in adults and the commonest causes for arrest are VF or pulseless VT. A witnessed cardiac arrest in these cases can be efficiently reverted with immediate defibrillation and cardiac compressions, which is life saving, and should be the goal in BLS.. In the A-B-C sequence, chest compressions are often delayed while the responder opens the airway to give mouth-to-mouth breaths, retrieves a barrier device,or gathers and assembles ventilation equipment.After initiating the emergency response system the next important thing is to start chest compressions.Only infant cpr is an exception to this protocol,where the previous sequence remains unchanged. That means no more looking, listening and feeling,as this component of assessment is removed from the guidelines. In the C-A-B sequence,chest compressions will be initiated sooner and ventilation only minimally delayed until completion of the first cycle of chest compressions. It was observed that the bystanders of the arrested victims do not actively participate in CPR as they find the first step of a-b-c sequence is difficult to perform. A-B-C starts with the most difficult procedures: opening the airway and delivering rescue breaths and that is the reason why less than one third of the victims in cardiac arrest receive by stander CPR in a witnessed cardiac arrest.. Hence a change in sequence to C-A-B 3.Compression rate: Should be at least 100/min (rather than“approximately” 100/min). The number of chest compressions delivered per minute during CPR is an important determinant of return of spontaneous circulation (ROSC) and survival with good neurologic function 4.Compression depth: For adults has been changed from the range of 1½ to 2 inches to at least 2 inches (5 cm).(The motto is push harder and faster) Effective compressions generate critical blood flow and oxygen and energy delivery to the heart and brain.
5.Hands Only CPR: Hands Only CPR. This is technically a change from the 2005 Guidelines, butAHA
endorsed this form of CPR in 2008. The Heart Association still wants untrained lay rescuers to do Hands Only CPR on adult victims who collapse in front of them.Hands-Only (compression-only) CPR is easier for an untrained rescuer to perform and can be more readily guided by dispatchers over the telephone.It was documented that survival rates from cardic arrest of cardiac origin are same irrespective of compressions alone(hands only cpr) or compressions with ventilations 5.Dispatcher Identification of Agonal Gasps: It is important that the rescuer shoul be well trained to identify between normal respirations from agonal breaths, in order to proceed with CPR. The lay rescuer should be taught to begin CPR if the victim is “not breathing or only gasping.” The healthcare provider should be taught to begin CPR if the victim has “no breathing or no normal breathing (ie, only gasping).”This rapid breathing check should be done before activation of emergency response system.
6.Cricoid Pressure: Routine use of cricoid pressure is not recommended as it may impede ventilation. Studies showed that cricoid pressure can delay or prevent the placement of an advanced airway and some aspiration can still occur even with proper application.In addition, it is difficult to appropriately train rescuers in use of this maneuver.
7.Activation of Emergency Response System: Should be made after assessment of the patients' responsiveness and breathing but should not be delayed. The 2005 guidelines states immediate activation of EMS after finding an unresponsive victim.(or send someone to do so), If the healthcare provider does not feel a pulse within 10 seconds, the provider should begin CPR and use the AED when it is available. 8. Concept of team resuscitation: For better and efficient delivery of resuscitation,is emphasized.
ELECTRICAL THERAPIES INCLUDING USE OF AED AND DEFIBRILLATOR.
1.AED Use in Children Now Includes Infants
For attempted defibrillation of children 1 to 8 years of age with an AED, the rescuer should use a pediatric
dose-attenuator system if one is available. If the rescuer provides CPR to a child in cardiac arrest and does not have an AED with a pediatric dose-attenuator system, the rescuer should use a standard AED. For infants (<1 year of age), a manual defibrillator is preferred. If a manual defibrillator is not available,an AED with pediatric dose attenuation is desirable. If neither is available, an AED without a dose attenuator may be used. Automated external defibrillators with relatively high-energy doses have been used successfully in infants in cardiac arrest, with no clear adverse effects. No other major changes have bee made in electrical therapies including AED and defibrillator.
ADVANCED CARDIAC LIFE SUPPORT 1.Capnography Recommendation: Quantitative waveform capnography is recommended for confirmation of endotracheal tube placement and for monitoring CPR quality and detecting return of spontaneous circulation based on end tidal CO2. Because blood must circulate through the lungs for CO2 to be exhaled and measured, capnography can also serve as a physiologic monitor of the effectiveness of chest compressions and to detect return of spontaneous circulation. Ineffective chest compressions (due to either patient characteristics or rescuer performance) are associated with a low Petco2 and return of spontaneous circulation is associated with an abrupt increase in ETCO2. Previously an exhaled carbon dioxide (CO2) detector or an esophageal detector device was recommended to serve this purpose. 2.Simplified ACLS Algorithm and New Algorithm: The new circular algorithm is introduced in 2010
The conventional ACLS Cardiac Arrest Algorithm has been simplified and streamlined to emphasize
the importance of high-quality CPR. The 2010 AHA Guidelines for CPR and ECC note that CPR is ideally guided by physiologic monitoring and includes adequate oxygenation and early defibrillation while the ACLS provider assesses and treats possible underlying causes of the arrest. There is no definitive clinical evidence that early intubation or drug therapy improves neurologically intact survival to hospital discharge.The algorithm focusses on to the basics with an increased emphasis on what is known to work: high quality CPR.
3.New Medication Protocols:
Atropine is not recommended for routine use in the management of PEA/asystole and has been removed from the ACLS Cardiac Arrest Algorithm.
The algorithm for treatment of tachycardia with pulses has been simplified. Adenosine is recommended in the initial diagnosis and treatment of stable,undifferentiated regular, monomorphic wide-complex tachycardia (this is also consistent in ACLS and PALS recommendations). It is important to note that adenosine should not be used for irregular wide-complex tachycardias because it may cause degeneration of the rhythm to VF.
4.Organized Post–Cardiac Arrest Care: 2010 (New): Post–Cardiac Arrest Care is a new section
in the 2010 AHA Guidelines for CPR and ECC. To improve survival for victims of cardiac arrest who are admitted to a hospital after ROSC, a comprehensive, structured, integrated,multidisciplinary system of post–cardiac arrest care should be implemented in a consistent manner.Treatment should include cardiopulmonary and neurologic support. Therapeutic hypothermia and percutaneous coronary interventions (PCIs) should be provided when indicated.Because seizures are common after cardiac arrest, an electroencephalogram for the diagnosis of seizures should be performed with prompt interpretation as soon as possible and should be monitored frequently or continuously in comatose patients after ROSC.
5.Initial and Later Key Objectives of Post–Cardiac Arrest Care:
1. Optimize cardiopulmonary function and vital organ perfusion after ROSC
2. Transport/transfer to an appropriate hospital or critical care unit with a comprehensive post–cardiac arrest treatment system of care
3. Identify and treat ACS and other reversible causes
4. Control temperature to optimize neurologic recovery
5. Anticipate, treat, and prevent multiple organ dysfunction.This includes avoiding excessive ventilation and hyperoxia.
6.Tapering of Inspired Oxygen Concentration:
After ROSC Based on Monitored Oxyhemoglobin Saturation, ie, SPO2. New recommendation
ETHICAL ISSUES
The ethical issues relating to resuscitation are complex,occurring in different settings (in or out of the hospital) and among different providers (lay rescuers or healthcare personnel) and involving initiation or termination of basic and/or advanced life support. All healthcare providers should consider the ethical, legal, and cultural factors associated with providing care for individuals in need of resuscitation. Although providers play a
role in the decision-making process during resuscitation, they should be guided by science, the preferences of the individual or their surrogates, and local policy and legal requirements.
Terminating Resuscitative Efforts in Adults With Out-of-Hospital Cardiac Arrest
• Arrest not witnessed by EMS provider or first responder
• No ROSC after 3 complete rounds of CPR and AED analyses
• No AED shocks delivered
For situations when ACLS EMS personnel are present to provide care; for an adult with out-of-hospital cardiac arrest, an “ACLS termination of resuscitation” rule was established to consider
terminating resuscitative efforts before ambulance transport if all of the following criteria are met:
• Arrest not witnessed (by anyone)
• No bystander CPR provided
• No ROSC after complete ALS care in the field
• No shocks delivered
Implementation of these rules includes contacting online medical control when the criteria are met. In 2005 guidelines,no specific criteria were established
THE PEDIATRIC ADVANCED CARDIAC LIFE SUPPORT
Many key issues in the review of the PALS literature resulted in refinement of existing recommendations rather than new recommendations;
1. Monitoring capnography/capnometry is again recommended to confirm proper endotracheal tube position and may be useful during CPR to assess and optimize the quality of chest compressions.
2.The PALS cardiac arrest algorithm was simplified to emphasize organization of care around 2-minute periods of uninterrupted CPR.
3.The initial defibrillation energy dose of 2 to 4 J/kg of either monophasic or biphasic waveform is reasonable but for ease of teaching, a dose of 2 J/kg may be used (this dose is the same as in the 2005 recommendation). For second and subsequent doses, give at least 4 J/kg. Doses higher than 4 J/kg (not to exceed 10 J/kg or the adult dose) may also be safe and effective, especially if delivered with a biphasic defibrillator.
4.On the basis of increasing evidence of potential harm from high oxygen exposure, a new recommendation has been added to titrate inspired oxygen (when appropriate equipment is available), once spontaneous circulation has been restored, to maintain an arterial oxyhemoglobin saturation ≥94% but <100% to limit the risk of hyperoxemia.
5.New sections have been added on resuscitation of infants and children with congenital heart defects,including single ventricle, palliated single ventricle, and pulmonary hypertension. The use of extracorporial membrane oxygenation , if facilities are available is stressed.
6.Several recommendations for medications have been revised. These include, not administering calcium except in very specific circumstances like hypocalcemia, calcium channel blocker overdose,
hypermagnesemia, or hyperkalemia. and limiting the use of etomidate in septic shock. Routine calcium
administration in cardiac arrest provides no benefit and may be harmful.
7.Indications for postresuscitation therapeutic hypothermia have been clarified somewhat.(see below)
8.New diagnostic considerations have been developed for sudden cardiac death of unknown etiology.
9.Providers are advised to seek expert consultation, if possible, when administering amiodarone or procainamide to hemodynamically stable patients with arrhythmias.
10.The definition of wide-complex tachycardia has been changed from >0.08 second to >0.09 second.
When a sudden, unexplained cardiac death occurs in a child or young adult, obtain a complete past medical and family history (including a history of syncopal episodes, seizures, unexplained accidents/drowning, or sudden unexpected death at <50 years of age) and review previous ECGs. All infants, children, and young adults with sudden, unexpected death should, where resources allow, have an unrestricted complete autopsy,
preferably performed by a pathologist with training and experience in cardiovascular pathology. Tissue should be preserved for genetic analysis to determine the presence of channelopathy. It is explained as ;There is increasing evidence that some cases of sudden death in infants, children, and young adults may be associated with genetic mutations that cause cardiac ion transport defects known as channelopathies. These can cause fatal arrhythmias, and their correct diagnosis may be critically important for living relatives
NEONATAL RESUSCITATION
1.Once positive-pressure ventilation or supplementary oxygen administration is begun, assessment should consist of simultaneous evaluation of 3 clinical characteristics:heart rate, respiratory rate, and evaluation of the state of oxygenation (optimally determined by pulse oximetry rather than assessment of color)
2. Anticipation of the need to resuscitate: during elective cesarean section
3. Ongoing assessment
4.Supplementary oxygen administration; For babies born at term, it is best to begin resuscitation with air rather than 100% oxygen.Administration of supplementary oxygen should be regulated by blending oxygen and air, and the amount to be delivered should be guided by oximetry.
5.Suctioning : There is no evidence that active babies benefit from airway suctioning, even in the presence of meconium, and there is evidence of risk associated with this suctioning. The available evidence does not support or refute the routine endotracheal suctioning of depressed infants born through meconium-stained amniotic fluid.
6.Ventilation strategies (no change from 2005)positive airway pressure may be helpful in the transitioning of the preterm baby. Use of the laryngeal mask airway should be considered if face-mask ventilation is unsuccessful and tracheal intubation is unsuccessful or not feasible.
7.Recommendations for monitoring exhaled CO2. Exhaled CO2 detectors are recommended to confirm endotracheal intubation.
8.Compression-to-ventilation ratio remains the same: The recommended compression-to-ventilation ratio remains 3:1. If the arrest is known to be of cardiac etiology, a higher ratio (15:2) should be considered.
9.Thermoregulation of the preterm infant should be considered (no change from 2005)
10.Postresuscitation therapeutic hypothermia: It is recommended that infants born at ≥36 weeksof gestation with evolving moderate to severe hypoxic-ischemic encephalopathy should be offered therapeutic hypo thermia.
11.Delayed cord clamping : There is increasing evidence of benefit of delaying cord clamping for at least 1 minute in term and preterm infants not requiring resuscitation. There is insufficient evidence to support or refute a recommendation to delay cord clamping in babies requiring resuscitation.
12.Withholding or discontinuing resuscitative efforts (Reaffirmed 2005 Recommendation): In a newly born baby with no detectable heart rate, which remains undetectable for 10 minutes, it is appropriate to consider stopping resuscitation,considering factors such as the presumed etiology of the arrest, the gestation of the baby, the presence or absence of complications, and the potential role of therapeutic hypothermia.
THERAPEUTIC HYPOTHERMIA
In adult post–cardiac arrest patients treated with therapeutic hypothermia, it is recommended that clinical neurologic signs, electrophysiologic studies, biomarkers, and imaging be performed where available, at 3 days after cardiac arrest. Currently, there is limited evidence to guide decisions regarding withdrawal of life support. The clinician should document all available prognostic testing 72 hours after cardiac arrest treated
with therapeutic hypothermia and use best clinical judgment based on this testing to make a decision to withdraw life support when appropriate. Explained as; on the basis of the limited available evidence, potentially reliable prognosticators of poor outcome in patients treated with therapeutic hypothermia after cardiac arrest include bilateral absence of N20 peak on somatosensory evoked potential more than or equal to 24 hours after cardiac arrest and the absence of both corneal and pupillary reflexes >3 days after
cardiac arrest. Limited available evidence also suggests that a Glasgow Coma Scale Motor Score of 2 or less at day 3 after sustained return of spontaneous circulation and presence of status epilepticus are potentially unreliable prognosticators of poor outcome in post-cardiac arrest patients treated with therapeutic hypothermia. Similarly, recovery of consciousness and cognitive functions is possible in a few post-cardiac arrest patients treated with therapeutic hypothermia despite bilateral absent or minimally present N20 responses of median nerve somatosensory evoked potentials, which suggests they may be unreliable as well. The reliability of serum biomarkers as prognostic indicators is also limited by the relatively few patients who have been studied.
DR.M KHAN SHERIEF,MBBS, DA, DNB.
POST GRADUATION IN ANAESTHESIOLOGY AND INTENSIVE CARE FROM THE PRESTIGIOUS MEDICAL COLLEGE KOTTAYAM,KERALA,INDIA AND PRESENTLY WORKING AS ANAESTHESIOLOGIST AND MEDICAL DIRECTOR AT LIFELINE HOSPITAL SOHAR,SULTANATE OF OMAN