

CEB is a commonly performed anaesthetic procedure to provide intra operative and postoperative analgesia in children undergoing lower limb and abdominal surgeries. It is a simple and highly effective technique useful for most of the surgical procedures of the lower half of the body, like urinary tract surgeries,circumcision, herniorrhaphies, orthopedic surgeries on the lower limb and pelvis, or operations of the anus or rectum.Excellent surgical conditions are obtained in congenital talipus equino varus(CTEV) surgery when combined with light general anaesthesia.The technique can be successfully used in children, as the fluidity of the epidural fat is more compared to adults, allowing easy spread of the deposited solution. Moreover if lumbar or thoracic anaesthesia is required, an epidural catheter can be threaded and advanced easily to achieve analgesia at the desired dermatomal level.
Anatomical Landmarks:


- The sacral and coccygeal nerves with their dorsal root ganglia
- The terminal part of the dural sac which ends between S1 and S3 and from where the pia mater extends downwards as filum terminale.
- A venous plexus formed by the extension of internal vertebral plexus.
- loose areolar and fatty tissue.
- The filum terminale - the terminal fibres of the spinal cord which does not contain nerves. This exits through the sacral hiatus and is attached posterior to coccyx.
The volume of the sacral canal averages 14.4 mL, but varies from 9.5 to 26.6 mL.
Drugs and dosages: Most commonly used drugs are lignocaine and bupivacaine Additives may be used to enhance analgesia, relaxation or prolongation of effect.For practical purposes the dosage suggested by Armitage may be used which is simple and easy to remember.
Armitage Formula:
Bupivacaine, max dose 2.5 mg/kg without adrenaline and 3mg/kg with adrenaline(1:200000)
0.5 ml/kg for a lumbosacral block
1 ml/kg for a thoraco-lumbar block
1.25 ml/kg for a midthoracic block
(0.25% Bupivacaine up to a maximum of 20ml, for analgesia and 0.5% if motor block is desired.)
Lignocaine max dose 7mg/kg without adrenaline and 10 mg/kg with adrenaline
0.5 ml/kg for lumbosacral block
1ml/kg for thoracolumbar block
1.5 ml/kg for mid thoracic block
(Maximum of 20ml, 1% for analgesia and 2 % for motor block)
If more than 1ml/kg (to a maximum of 20 ml) needs to be given it is preferable to avoid caudal route and go for a higher epidural route(for lesser volume of drug) as it is observed that large volumes of caudal drug spread rostrally above T4. According to bromage;[2] anesthetic dose requirements are about 0.1 mL/ segment/year of age for 1% lidocaine or 0.25% bupivacaine.

Scott’s Calculation:
Calculates the dose based on the child’s age and/or weight table.If the child is of average weight for his or her height, both figures will be the same.Avoid this formula in obese children to prevent overdosage.
Identification of the sacral hiatus and the procedure of the block:
The procedure must be carried out under strict aseptic precautions, Patient position:
Lateral position in children or prone position (desirable) for adults.The pelvis is elevated with the help of a pillow and the thighs are little extended The legs turned in wards,(internally rotated ). This makes the identification of the hiatus more easy by relaxing gluteal muscles. Look at figure 2B.
The standard technique as described by Miller is shown below:[3]
Caudal anesthesia requires identification of the sacral hiatus. The sacrococcygeal ligament (i.e.,extension of ligamentum flavum) overlying the sacral hiatus lies between the sacral cornua. To facilitate locating the cornua, the posterior superior iliac spines should be located and, by using the line between them as one side of an equilateral triangle, the location of the sacral hiatus should be approximated After the sacral hiatus is identified, the index and middle fingers of the palpating hand are placed on the sacral cornua,
and the caudal needle is inserted at an angle of approximately 45 degrees to the sacrum.

While advancing the needle, a decrease in resistance to needle insertion should be appreciated as the needle enters the caudal canal. The needle is advanced until bone (i.e., dorsal aspect of the ventral plate of the sacrum) is contacted and then slightly withdrawn, and the needle is redirected so that the angle of insertion relative to the skin surface is decreased. In male patients, this angle is almost parallel to the coronal plane; in female patients, a slightly steeper angle (15 degrees) is necessary. During redirection of the needle and after loss of resistance is again encountered, the needle is advanced approximately 1 to 2 cm into the caudal canal.


Performance of caudal block.[6] SC, sacral cornua; PSIS, posterior superior iliac spine; SH, sacral hiatus; TC, tip of coccyx. Note that an equilateral triangle is formed with the fingertips from PSIS to PSIS to needle insertion at SH.(By courtesy of Cristian TANASE,Clinical Emergency Hospital for Children “Grigore Alexandrescu” Bucharest.)

Further advance is not attempted because dural puncture and unintentional intravascular cannulation become more likely. One method of increasing the likelihood of correct caudal needle placement is to inject 5 mL of saline rapidly through the caudal needle while palpating the skin overlying the sacrum. If no midline bulge is detected, the needle is probably positioned correctly. In contrast, if a midline bulge is detected during saline injection, the needle is positioned incorrectly.
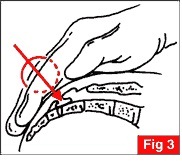
1).Palpate the coccyx with the index finger of the left hand
2).Slide the palpating finger cephalad
3).Feel the depression.
4).Keep the finger at the hiatus and turn the hand at 80 degrees anchoring the index finger at the hitus
5).Hold the syringe filled with the drug in right hand.

1)Pierce the SC ligament by entering into it at 45 degree angle
2)Carefully advance and feel for the "click"
3)Once the click is felt lower the needle almost parallel to the coronal plane (along the long axis of the spinal canal)
4)Advance the needle further 1-2 cm into the caudal canal.
Instead of using the needle alone , a syringe filled with 1-2 ml saline may be attached to it.Once the caudal canal is entered, the saline can be injected freely without any resistance. Air should not be used for this loss of resistance technique as the incidence of air embolism is high in children.Once the canal is identified local anaesthetic test dose may be given to rule out accidental intravascular or dural puncture.
Continuous caudal anaesthesia may be given by inserting an epidural catheter through an indwelling cannula or a 20 gauge touhy needle used to puncture.Remember that the catheter can be threaded easily because of the fluidity of loose areolar tissues in children and catheter tip in mid thoracic or higher level may lead on to a higher level of block.Measuring the catheter with the length of spine may be used as a rough guide to decide on how far the catheter to be inserted.Tunnelling the catheter on the back using a touhy needle helps to secure the catheter and prevent fecal contamination of the entry site as well.
How to identify the caudal space and to ensure the correct placement of catheter.
- Ease of injection by loss of resistance technique
- Absence of a cutaneous bulging over the injection site
- Test dose, A small amount of local anaesthetic should be injected as a test dose (2-4mls).Look for peri oral tingling or numbness,or hypotension Also look for lower lumbar segment motor block. If the test is negative proceed with injection.
- Aspiration test for either CSF or blood.[2] A negative aspiration test does not exclude intravascular or intrathecal placement. The injection rate should not exceed 10 ml/30 seconds.[3] During injection also watch for acute toxicity
- The whoosh test and modified swoosh test(see below)
- Flouroscopy(see below)
- Nerve stimulation test,the presence or absence of anal sphincter contraction to electrical stimulation is used as a guide for correct needle placement (using epidural nerve stimulators)
- Ultrasound.(see below)
The whoosh test and modified swoosh test:[4]
The whoosh test is done by injection of air into the caudal epidural space with simultaneous auscultation over the thoracolumbar spine for an audible "whoosh" sound.Injection of air is associated with side effects like neurological complicaions and air embolism. So is being replaced by swoosh test where saline or the LA solution is used instead of air.1-1.5 ml of air or saline is used.
Fluoroscopy: is most commonly used in interventional spine procedures and is frequently used in confirming the location of caudal epidural needle[6]. It is necessary that caudal epidural needle placement should be confirmed by fluoroscopy alone or by epidurography when the procedure is used for caudal epidural injection of steroids for treating chronic pain syndromes.

Ultrasound: Combined with fluoroscopy ultrasound gives almost 100% accuracy in placement of the needle.As an adjuvant tool ultrasound is useful along with other methods in difficult cases and when successful placement is mandatory.Ultrasound is radiation free, is easy to use, and can provide real-time images in guiding the caudal epidural needle into the caudal epidural space.[6]Sterile precautions are taken before probe placement and a transverse view of the sacral hiatus is made first by placing the transducer transversely at the midline over hiatus.The hiatus is seen as a hypoechoic region between two hyper echoic shadows, the SC ligament and the dorsal bony surface. Then a longitudinal view is made by keeping the transducer between the sacral cornua,and a needle is inserted and advanced under sonographic guidance in real time.The portion of the needle which entered into the canal may not be seen clearly.Again the transducer is rotated to view the transverse axis where the needle tip may be visualised as a small round hyper echoic structure between the two hyperechoic cornua and within the two hyper echoic bands formed by the SC ligament and the dorsal bony wall of sacrum.
Images below are reproduced from Chen, Carl P. C. M.D.; Tang, Simon F. T. M.D,Anesthesiology:July 2004 - Volume 101 - Issue 1 - pp 181-184[7] where a detailed description of the procedure is available


Adjuvants used along with Local Anaesthetics: Adjuvants are used to intensify the block ,to reduce systemic absorption or to prolong the action.The commonly used adjuvants are,
Opioids :Prolong analgesia in infants and children but with attendant risks of respiratory depression and side effects like nausea vomiting and itching. It can produce urinary retention also. Hence morphine administration should be done under monitoring of vitals. Catheterization may sometimes be required. A dose of 50mcg/kg of preservative free morphine or diamorphine 30mcg/kg can be added to the local anesthetic solution[8].The optimal dose is between 33-50 μg/kg.[9] This will provide 12 to 24 hours of analgesia.Fentanyl 1-2 ug/kg may be also used but with unpredictable duration of action.
Clonidine: An α2-adrenergic agonist,. A dose of 0.5-1.0 microgram/kg improves the quality and duration of analgesia without significant side effects[8]The analgesia may last upto 12 hours.Sedation and bradycardia are noted at doses above 5mic/kg.
Ketamine: An NMDA antagonist. In doses of 0.25 - 1.0 mg/kg, causes significant prolongation of post operative analgesia, without significant side effects. May be combined with 0.25%bupivacaine.Preservative free ketamine is preferred. Higher doses (>0.5mg/kg) may produce neuroleptic side effects
Epinephrine: 5 mic/ml of epinephrine is used to detect intravascular placement of catheter or needle.It also prolongs the duration of action of LA by local vasoconstriction and thereby delaying uptake and metabolism.
Continuous epidural anaesthesia: is possible by inserting a catheter into the caudal space, through an indwelling cannula or a touhy needle.The initial dose may be 0.05ml/seg/kg[10]
- Less than 1 year of age 0.1-0.2ml/kg/hr of 0.1% bupivacaine
- more than 1 year 0.1% bupivacaine with 3 microgram/ml of fentanyl at the rate of 0.1-0.4ml/kg/hr, (less than 0.5microgram/kg/hr of fentanyl to start with.)[11]Ropivacaine is used at the dose of 0.4mg/kg/hr
Pharmacological Considerations:
Local anaesthetics are classified into two groups, amides and esters. the amides are metabolised in liver while the esters are hydrolysed by esterases in the plasma.Since newborn and pediatric liver functions are immature and not fully functional the metabolism of amides is not complete and the un metabolised fraction can produce toxic reactions. Another factor which contributes to toxicity is the reduction in plasma proteins like albumin and alpha 1 acid glycoprotein resulting in excess free fraction of the drugs in plasma. On the contrary the volume of distribution of local anaesthetics is more in children compared to adults causing a reduction plasma concentrarion of these drugs and which may nullify the effect of reduced elimination allowing higher doses.For eg:The maximum safe dose of bupivacaine in neonates is 1.5mg/kg.Other Local anaesthetic drugs which may be used for caudal include Ropivacaine 0.2- 2 mg/kg and Levobupivacaine 0.25- 1 mg/kg with slight increase in duration of action.Pregnant patients need 25-35% reduction in dose requirements for labour analgesia due to engorged epidural veins reducing space.Caudal blockade in pediatrics is used primarily for perioperative pain control, whereas in adults it is primarily for chronic pain management. [12]

Combination with GA: For intra and post operative pain relief and to reduce the requirement of depressant general anaesthetic agents for rapid and smooth recovery, caudal is combined with GA, The procedure is ideal for children as positioning after induction is easy and the success rate is high. Inhalational or iv induction then securing airway with LMA or ETT, is followed by caudal injection.The disadvantage being, failure of detection of LA toxicity or high block in an anaesthetised child.Careful monitoring of vitals mandatory.The effectiveness of the block is determined by "loss of anal sphincter tone".[13]
Indications(Uses) :
- Apart from the usual indications mentioned above the caudal block is highly useful for emergency surgical procedures like,testicular torsion, omphalocele correction,strangulated hernias,high risk neonates for anorectal and abdominal surgeries,biliary tract surgeries and operative procedures on stomach (especially when a catheter is threaded to deposit the drug at higher dermatomes)
- Ambulatory and day care minor surgeries where fast-traching is desired.
- For combining with General anaesthesia to provide stable hemodynamics, adequate analgesia and to reduce the requirement of general anaesthetic agents, in surgeries of abdomen, lower thorax or even open heart procedures.
- Continuous epidural analgesia can be provided with a catheter in caudal space for long surgical procedures like orthopedic corrective surgeries or plastic surgery procedures of the lower limb.
- Percutaneous epidural neuroplasty is a technique of administering local anesthetics, corticosteroids, hyaluronidase, and hypertonic saline through a caudal catheter for the purpose of lysing epidural adhesions. [13]
Advantages over conventional epidural anaesthesia:
- Easy location because of the prominent anatomical landmarks, helps to establish the block faster
- Reduced incidence of failed or patchy blocks
- Predictable distribution of LA solution
- Easy to place a catheter
Side effects:
- Failed block , the incidence is as high as 5-20%.Ultrasound guidance helps to increase the success rate
- Predominant unilateral block or patchy block. Lateralisation is due to rapid injection.
- Dural puncture: due to anatomic variation and low lying dura in infants. Sequale is, a total spinal block with dilated pupils, apnea, and unconsciousness.
- Local anaesthetic toxicity can be either due to intravascular injection or due to overdose resulting in excess plasma concentrations.Since the extradural veins have no valves, retrograde flow is fast once the drug is injected intravascularly.
- Intra osseous injection
- Bleeding
- Introduction of infection.
Contraindications:
- Patient refusal
- local infections,eg: dermattis, pilonidal sinus
- Coagulation disorders
- Neurologic diseases,Poliomyelitis
- Sensitivity to local anaesthetics
- Increased intra cranial tension like meningitis, hydrocephalus etc.
- Congenital malformations of lower meninges or spine eg: spina bifida, meningo myelocele
- Unstable cardiovascular system, valvular heart diseases
Management of Local Anaesthetic toxicity( in general:)[4]
- Oxygenation, intubation, cardiac massage
- Sodium bicarbonate hypertonic 4.2%(through central vein preferably) 2ml/kg/10 mts.(1mmol/kg/10mt) or isotonic 1.4% through peripheral vein 6ml/kg/10 mts(1mmol/kg/10mts)
- IV midazolam or diazepam for seizures
- IV atropine 0.02mg/kg
- IV vasoactive agents, epinephrine 0.1ml/kg1/10000 solution (10 microgram/kg) or isoprenaline 0.1 mic/kg
- Dopamine or dobutamine infusion 2-10 mic/kg/mt,
- Calcium chloride 10-30 mg/kg
- Treatment of VF/VT as per ACLS guidelines
- Lipid emulsions IV.
Role of caudal block in pain management:
In radiculopathies refractory to routine management this route is adopted for pain relief. Percutaneous epidural neuroplasty uses a caudal catheter left in place for up to 3 days to inject hypertonic solutions into the epidural space to treat radiculopathy with low back pain and epidural scarring, typically from previous lumbar spinal surgery.[12]After confirmation of epidural space by fluoroscopy a mixture of drugs consisting of Local anaesthetics, steroids, hyaluronidase, and saline is injected.Initially1500 units ofhyaluronidase in 10mLof preservative-free saline is injected rapidly. This is followed by an injection of 10 mL of 0.2% ropivacaine and 40 mg of triamcinolone, An additional injection of 9 mL of 10% hypertonic saline is infused over 20 to 30 min. On the second and third days, the local anesthetic (ropivacaine) injection is followed up by the hypertonic saline solution. Antibiotic coverage is provided to reduce the possibility of epidural abscess formation.[12]. The video below illustrates how to conduct an ultrasound guided epidural instillation of steroids to treat chronic pain syndromes. Reference:
1).NJH Davies, JN Cashman, Lee's Synopsis of Anaesthesia 13 th edition, Butterworth Heineman2).Bromage PR: Epidural Analgesia. WB Saunders, 1978, pp 258-282
3).Dr.Bela Vadodaria and Dr David Conn, "Update in Anaesthesia" Issue 8 (1998) Article 3: http://www.nda.ox.ac.uk/wfsa/html/u08/u08_011.htm
4).Ronald D Miller; Millers anaesthesia, 7th edition, Churchil Livingstone
5).Anaesthesia.1998 Aug;53(8):829. http://www.ncbi.nlm.nih.gov/pubmed/9797541
3).Dr.Bela Vadodaria and Dr David Conn, "Update in Anaesthesia" Issue 8 (1998) Article 3: http://www.nda.ox.ac.uk/wfsa/html/u08/u08_011.htm
4).Ronald D Miller; Millers anaesthesia, 7th edition, Churchil Livingstone
5).Anaesthesia.1998 Aug;53(8):829. http://www.ncbi.nlm.nih.gov/pubmed/9797541
6). Cristian TANASE, www.umftgm.ro/d_ati/.../Neuraxial%20blocks_engl.pdf
7)..Chen, Carl P. C. M.D.; Tang, Simon F. T. M.D, Pain and Regional AnesthesiaUltrasound Guidance in Caudal Epidural Needle Placement, Anesthesiology:July 2004 - Volume 101 - Issue 1 - pp 181-1848).Alice Edler MD, MA,Vinit G.Wellis, MD, Caudal Epidural Anaesthesia for paediatric patients,Update in Anaesthesia 1998 No. 8
9).Krane EJ, Tyler DC, Jacobson LE. The dose response of caudal morphine in children. Anesthesiology 1989; 71:48-52.
10.Amr aboulesh(anesthesiology 79:400,1993,) www.cmuh.org.tw/HTML/dept/.../20081119_pedi_regional.pp
11).Amr aboulesh(anesthesiology 79:400,1993,) www.cmuh.org.tw/HTML/dept/.../20081119_pedi_regional.pp.(anesthesia analgesia 75:164, 1992)
12).Kenneth D. Candido, MD and Alon Winnie, MD, Caudal Anaesthesia,;Paediatr Anaesth 2003; 13:31 1317.
13).Verghese S, Mostello L, Patel R: Testing anal sphincter tone predicts the effectiveness of caudal analgesia in children. Anesth Analg 2002:94:1161-1164.













7 comments:
AERW79Q8FZH3
hello dr sherief khan .i give lot of caudal epidural. this review was very useful. keep the good work
one great review.......and the complications are very well dealt...
Hey
Absolutely brilliant.
really helpful.
you have done some research. Brilliant.
please also read my blog:
http://kratik1987.blogspot.com/
Cheers :)
Kratik
Hey
Absolutely brilliant.
really helpful.
please also read my blog:
http://kratik1987.blogspot.com/
Cheers :)
Kratik
Hi Doctor, you are serving the community very well. I am dr subodh and i also run a similar site called http://kakinadaedu.in
I was looking for similar sites and found yours. i have posted a link of your site to mine also. Pls keep up the good work and do mail me back. may be we can contribute to each other's work
Post a Comment